Tag Motor Neuron Disease

Tag Motor Neuron Disease: Understanding the Progressive Neurological Disorder
Motor neuron disease (MND), a group of progressive neurodegenerative disorders, disrupts the function of motor neurons, the nerve cells responsible for controlling voluntary muscle movement. While the term "MND" encompasses several distinct conditions, amyotrophic lateral sclerosis (ALS) is the most common and well-known form. This article will delve into the intricacies of MND, focusing on its underlying mechanisms, diverse presentations, diagnostic challenges, and current therapeutic approaches, aiming to provide a comprehensive overview for both medical professionals and individuals seeking detailed information about this debilitating condition. Understanding MND is crucial for improving patient care, advancing research, and ultimately, finding effective treatments.
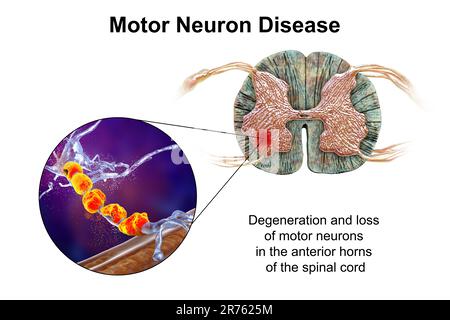
The core pathology of MND lies in the degeneration and eventual death of motor neurons in the brain (upper motor neurons) and spinal cord (lower motor neurons). Upper motor neurons originate in the motor cortex of the brain and descend through the spinal cord, relaying signals to lower motor neurons. Lower motor neurons, located in the brainstem and spinal cord, directly innervate skeletal muscles. When either of these neuron types is affected, the communication pathway between the brain and muscles breaks down, leading to progressive muscle weakness, atrophy, and functional impairment. The loss of motor neurons is thought to be a complex interplay of genetic predispositions, environmental factors, and cellular dysfunction. Oxidative stress, excitotoxicity, protein misfolding and aggregation, mitochondrial dysfunction, and impaired axonal transport are all implicated mechanisms contributing to motor neuron death. The specific combination and dominance of these pathways can vary between different subtypes of MND, contributing to the heterogeneity of the disease.
The clinical manifestations of MND are diverse and depend on which population of motor neurons is primarily affected. The most prevalent form, ALS, typically involves a combination of upper and lower motor neuron signs. Upper motor neuron signs include spasticity (muscle stiffness and exaggerated reflexes), hyperreflexia, and a positive Babinski sign (an abnormal reflex where the toes fan out when the sole of the foot is stroked). Lower motor neuron signs, on the other hand, manifest as muscle weakness, fasciculations (involuntary muscle twitching), muscle atrophy (wasting), and flaccid paralysis. The onset of symptoms is usually insidious, with individuals initially noticing subtle difficulties such as tripping, dropping objects, or changes in voice or swallowing. As the disease progresses, these symptoms worsen, impacting increasingly larger muscle groups. The pattern of muscle involvement can also vary, with some individuals experiencing weakness primarily in the limbs (limb-onset MND), while others are affected more significantly by bulbar muscles controlling speech, swallowing, and breathing (bulbar-onset MND). This variability in presentation underscores the importance of a thorough clinical assessment.
Beyond ALS, other forms of MND exist, though they are rarer. Primary lateral sclerosis (PLS) primarily affects upper motor neurons, leading to progressive spasticity and weakness but without significant lower motor neuron involvement. Progressive muscular atrophy (PMA) predominantly impacts lower motor neurons, resulting in progressive muscle weakness and atrophy without prominent upper motor neuron signs. Pseudobulbar palsy (PBP) is another subtype characterized by bulbar dysfunction due to upper motor neuron damage, leading to difficulties with speech and swallowing but typically with preserved limb strength. The distinction between these subtypes is important for prognostication and, in some cases, for guiding management strategies, though the underlying pathological processes can share commonalities.
Diagnosing MND is a challenging process due to its progressive nature, the wide spectrum of symptoms, and the absence of a definitive diagnostic biomarker. The diagnosis is primarily clinical, relying on a comprehensive neurological examination to identify the characteristic signs of upper and lower motor neuron involvement. A detailed medical history, including the onset and progression of symptoms, is crucial. Electromyography (EMG) and nerve conduction studies (NCS) are essential diagnostic tools that help assess the electrical activity of muscles and nerves, detecting signs of denervation (loss of nerve supply to muscles) and confirming lower motor neuron dysfunction. Magnetic resonance imaging (MRI) of the brain and spinal cord is often performed to rule out other conditions that can mimic MND, such as spinal cord compression, tumors, or multiple sclerosis, which can present with neurological deficits. Blood tests are used to exclude other conditions that might cause muscle weakness, such as thyroid disorders or vitamin deficiencies. In some instances, genetic testing may be considered, particularly if there is a family history of MND, to identify mutations in genes associated with familial forms of the disease. However, for the majority of sporadic MND cases, genetic testing is less likely to yield a definitive diagnosis.
Currently, there is no cure for MND. Treatment focuses on managing symptoms, slowing disease progression, and improving the quality of life for individuals affected by the disorder. Riluzole, an oral medication, is the only drug approved by the U.S. Food and Drug Administration (FDA) for treating ALS. It is thought to work by reducing the release of glutamate, an excitatory neurotransmitter that can be toxic to motor neurons. While riluzole has been shown to modestly prolong survival, it does not reverse or halt the disease process. More recently, edaravone, an antioxidant administered intravenously, has also received FDA approval for ALS treatment, showing some benefit in slowing functional decline. Beyond pharmacological interventions, supportive care plays a critical role. Physical therapy aims to maintain muscle strength and mobility, prevent contractures, and adapt to functional limitations. Occupational therapy assists with adapting daily living activities and recommending assistive devices. Speech therapy addresses communication difficulties and swallowing problems, often involving strategies for modified speech and dietary recommendations to prevent aspiration. Nutritional support is paramount, as many individuals with MND experience weight loss and difficulty eating. Gastrostomy tube feeding may become necessary to ensure adequate calorie and fluid intake. Respiratory management is a significant concern as the disease progresses, impacting breathing muscles. Non-invasive ventilation, such as bilevel positive airway pressure (BiPAP), can help support breathing and improve sleep quality. In advanced stages, a tracheostomy and mechanical ventilation may be considered. Palliative care and hospice services are vital for providing comfort, managing pain and other distressing symptoms, and offering emotional and psychosocial support to patients and their families.
Research into the underlying mechanisms of MND is rapidly advancing, offering hope for future therapeutic breakthroughs. Gene therapy, aimed at correcting or replacing faulty genes responsible for familial MND, is an active area of investigation. Stem cell therapy, exploring the potential of replacing damaged motor neurons with healthy cells, is also being pursued, though significant challenges remain in ensuring cell survival, integration, and functional restoration. Drug development is focused on targeting various pathways implicated in motor neuron degeneration, including reducing inflammation, clearing protein aggregates, and enhancing neuroprotection. Clinical trials are constantly evaluating novel treatment strategies, offering patients access to cutting-edge research. The complex nature of MND necessitates a multi-pronged approach to research, encompassing basic science discoveries, preclinical studies, and rigorous clinical trials. Collaboration between researchers worldwide and patient advocacy groups is crucial for accelerating progress.
The genetic underpinnings of MND are becoming increasingly understood. While most cases of MND are sporadic (occurring randomly without a family history), approximately 5-10% are familial. Several genes have been identified as being associated with familial MND, including C9orf72, SOD1, FUS, and TARDBP. Mutations in these genes can lead to the production of toxic proteins that accumulate in motor neurons, triggering a cascade of cellular damage. The C9orf72 gene mutation is the most common genetic cause of familial ALS and FTD (frontotemporal dementia), highlighting the overlap between these neurodegenerative disorders. Understanding these genetic links not only provides insights into the disease mechanisms but also opens avenues for developing targeted therapies. For individuals with a family history of MND, genetic counseling can be beneficial to assess their risk and discuss potential implications.
The impact of MND extends beyond the physical debilitation. The neurological and functional decline significantly affects a person’s emotional and psychological well-being. Depression, anxiety, and feelings of isolation are common among individuals with MND and their caregivers. Therefore, comprehensive psychosocial support is an integral part of managing the disease. Support groups, counseling services, and access to mental health professionals are crucial for addressing these challenges. Open communication with healthcare providers about emotional concerns is vital. Caregiver burden is also a significant consideration. The progressive nature of MND often necessitates round-the-clock care, placing immense physical, emotional, and financial strain on family members and loved ones. Respite care services and access to resources for caregivers are essential to prevent burnout and ensure their well-being.
The journey with MND is profoundly challenging for patients and their families. While a cure remains elusive, significant strides are being made in understanding the disease, improving symptom management, and developing novel therapeutic strategies. Continued research, coupled with compassionate and comprehensive care, offers the best hope for improving the lives of individuals affected by this devastating neurological disorder. Public awareness and support for MND research initiatives are critical in driving progress towards effective treatments and, ultimately, a cure. The ongoing commitment to unraveling the complexities of MND promises a brighter future for those living with this progressive condition.







{kind=link}